Communities in Madagascar face numerous barriers in accessing diagnostics services. In this rapid assessment, led by Matahari Global Solutions, in partnership with the community-based organisation Ankizy Gasy, and supported by FIND, 43 individuals living in rural and semi-rural communities in Madagascar were interviewed to understand availability of diagnostics, and to understand barriers to accessing diagnostics.
This rapid assessment found a complex diagnostics environment marked by high out-of-pocket spending for diagnostics relative to income, relatively long distances to get to primary healthcare centres, doctors prescribing antibiotics with incomplete diagnostics regimens or no diagnostics at all, poor clinical practices on diagnostics (such as use of inaccurate terminology), and insufficient data about stockouts. Because rapid malaria tests are provided for free, doctors offer these more regularly, but upon a negative result are unable to recommend additional tests because of the cost barrier. The assessment also found that rural communities overwhelmingly wanted more accessible and affordable testing – and perceived that people they knew were dying from ‘unknown diseases’.
To learn more about the results of the assessment, and recommendations to address the barriers revealed, click below.
The COVID-19 pandemic exposed global gaps in testing for communicable and noncommunicable diseases, and these gaps disproportionately affect individuals and families in low- and middle- income countries (LMICs). A staggering 81% of the population in LMICs don’t have access to many of the most simple tests available (Lancet, 2021).1
UNICEF has responded to this global gap in testing by developing the “Let’s Test” Toolkit, which aims to support Advocacy Champions in their goal to increase the use of quality testing in their own communities, through both increased supply and demand generation. This Toolkit, utilizing evidence based strategies, provides step-by-step guides and assets to support impactful and productive engagement with policymakers to advocate for increased supply of quality testing. Communications assets, facilitation tools, memorable info-bites and content for social media campaigns are also provided to drive informed community-level demand and use of quality testing in LMICs.
The “Let’s Test” Toolkit has been informed by research in five LMICs and was designed with consideration for global health best practices for engagement, advocacy and social behavior change communication (SBCC). Practical guidance is also included to enable users of the Toolkit to tailor advocacy and communication assets for specific country and community contexts.
Access the Toolkit here to learn more: lets-test.org.
1 Lancet Commission on Diagnostics: transforming access to diagnostics (2021)
The Transition Report includes a summary of achievements against each transition objective, related monitoring and coordination activities (e.g., supported by the ACT-A Tracking and Monitoring Task Force), and a Pillar-by-Pillar update on implementation progress. It reflects inputs from across the ACT-A partners as well as from recent reports and meetings, including the 3rd meeting convened by the ACT-A Council Tracking and Monitoring Task Force on 31 March 2023.
Reflections on the way forward are provided in the final section of the report, with quarterly information (for Q4 2022 and Q1 2023) included as annexes. It also provides insights into how ACT-A partners have mainstreamed their COVID-19 work and will carry forward ongoing activities as part of their regular programmes and support.
The ACT-Accelerator Reflections Compendium features voices from across the partnership, reflecting on the experiences, successes and challenges of this unprecedented global collaboration and highlighting important learnings for the future from those who were involved in a variety of capacities. Key stakeholders including Facilitation Council member countries and regional entities, partner agencies, envoys, civil society and industry representatives, donors and others share their thoughts on ACT-A. Additionally, the compendium includes six country stories that demonstrate the work of the partnership in Sierra Leone, Cambodia, Peru, Lebanon, Zimbabwe, Philippines and Mongolia, focusing on areas such as expanding access to medical oxygen, accelerating vaccine delivery and advocating for self-testing.
This report is an outcome of the third meeting of the ACT-Accelerator Tracking and Monitoring Taskforce, held on 31st March 2023. This taskforce – co-chaired by India and the United States – continues key elements of the work of the Facilitation Council and its working groups. The report includes an outcome statement by the Co-Chairs and provides a briefing on the current status of the rollout of COVID-19 tools, including the institutional arrangements being put in place by ACT-A agencies to ensure ongoing access to COVID-19 tools. More information on the taskforce can be found here.
This report is an outcome of the second meeting of the ACT-Accelerator Tracking and Monitoring Taskforce, held on 15th February 2023. This taskforce – co-chaired by India and the United States – continues key elements of the work of the Facilitation Council and its working groups. The report includes an outcome statement by the Co-Chairs and provides a briefing on the current status of the rollout of COVID-19 tools, including the institutional arrangements being put in place by ACT-A agencies to ensure ongoing access to COVID-19 tools. More information on the taskforce can be found here.
Rapid diagnostic tests (RDTs) based on lateral flow assays have emerged as important diagnostic tools in the management of diseases such as malaria and COVID-19. However, errors can arise when individuals perform these tests and interpret their results. Mobile smartphone applications (apps) for reading RDTs offer a promising option to improve the accuracy of the interpretation of test results. This has been demonstrated with hardware RDT readers in low- and middle-income countries (LMICs). With apps, however, no additional hardware is needed, apart from a smartphone. Such smartphones are already becoming widely available, avoiding cost, supply chain, and maintenance concerns that would occur if new hardware needed to be deployed to read RDTs.
The aim of this report is to share a summary of publicly available information about mobile applications for reading RDTs. The focus is on RDT-reading apps that do not require additional hardware beyond a mobile device (meaning a smartphone or tablet) and the RDT kit. Apps for diseases of poverty and low-resource settings are of particular interest, but the report also includes other apps, to support an understanding of this industry overall.
Rapid diagnostic tests (RDTs) have played a critical role in the global COVID-19 response, as well as in the management and diagnosis of other diseases, such as malaria and HIV. However, without correct performance of the test and interpretation of the result, the utility of these tests may be compromised, presenting timely and accurate clinical assessment and disease surveillance.
This Target Product Profile lays out minimal and optimal characteristics for RDT readers to serve as companion tools to support improved test performance, interpretation, and reporting.
Rwanda has raised the bar in using digital tools to scale up community-based testing in its COVID-19 response.
A national Joint COVID Task Force, established in February 2020 before the first case was confirmed, led the pandemic response of this African country. The team gave both high-level strategic guidance and day-to-day operational support.
This had, however, been preceded by years of investment in the broader digital health infrastructure, where digital technologies were expanded to support service delivery – a longstanding government priority.
Institutions in Rwanda were therefore able to combine resources and capacities to respond to emerging problems. Adopting a multi-sectoral approach from the start has allowed rapid deployment of interventions and more efficient troubleshooting.
It also helped the country to build COVID-specific digital systems to strengthen the areas of testing, contact tracing, patient support and surveillance.
Rwanda’s numbers
First registered COVID-19 case: 14 March 2020 14 March 2021: more than 20 000 cases diagnosed, with mortality rate of 1.4%
Sharpest peak in cases: late 2020 and early 2021. This prompted stringent restrictions on movement that led to a rapid decline in new cases.
Testing the toolbox
Rwanda has used District Health Information Software (DHIS-2) to survey and monitor disease since 2011 and, in early 2020, this system was adapted to capture data on COVID-19 diagnosis and case management.
DHIS-2 is integrated with the laboratory information system which allows for automated transmission of data.
COVID-19 Command Posts, the sub-national operational centres of the Joint COVID Task Force, receive and analyse surveillance data from these different systems to inform policy and programme decisions.
Rwanda also devised a stringent port of entry system to avoid importing COVID-19 cases.
Other technologies were deployed in selected settings, including the internal Visitor Tracking Record and the e-ASCOV pilot, a locally developed application to help give access to rapid antigen testing.
Patient-facing tools
WhatsApp help line
Unstructured supplementary service data (USSD) platform, which provides basic information on COVID-19 on any phone with no data or airtime requirements
WelTel app, where patients can report symptoms
Standard electronic medical record (EMR) system
Online results portal
Open Data Kit (ODK) application which captures data for targeted surveillance activities outside of health facilities, particularly in hotspots.
Impact of digital tools
The use of digital tools in Rwanda has had a significant impact. For example, through integrating laboratory and health management information systems, the testing process is now paperless. All facilities capture data in the same central system.
Patient unique health codes (UHCs) also allow data transfer between different digital solutions. This cuts down the time taken by health care workers to record and report data, as it is captured in real-time at the point of care.
Application programming interfaces have also been developed for a number of tools to enable interoperability.
Mobile-data collection tools for community-based surveillance have generated valuable insights to inform timely responses to outbreaks.
Monitoring cases and contacts remotely using digital tools has reduced the burden on the health system. This has allowed the country to focus limited capacity on delivering services to the most at-risk individuals, while consistently monitoring other patients.
Key success factors in Rwanda
Pre-existing digital infrastructure
Political will, with digital infrastructure bolstered by political commitment at the highest levels of government
National ownership of systems, minimising the challenge of isolated pilots, duplicate interventions and “data fog”
Building on existing tools
Multisectoral collaboration
Providing patients with direct access to results.
Challenges
The lack of readiness of health care workers to adopt new digital tools can be a barrier to successful implementation.
This is worsened in a crisis such as COVID-19, where systems are already overwhelmed with new protocols and interventions.
Resource requirements are also unpredictable due to the rapidly evolving nature of the pandemic.
It is important to coordinate decisions on selection of digital tools from among numerous vendors.
KEY INSIGHTS
Ensuring integration of national COVID-19 data (public and private sector) into one platform enhances understanding of the pandemic and simplifies data management.
Leveraging databases in other areas can minimise the time and effort required for individual data capture.
Digital tools, particularly on mobile devices, are key in providing decentralised testing services.
While Rwanda is still in the early stages of rolling out its approach, it shows potential to expand and standardise testing outside of health facilities.
Integrating data into one platform: a better analysis of the cascade of care
Nigeria’s experience containing the Ebola epidemic of 2014 highlighted the critical need for a comprehensive data management system to deal with health outbreaks.
Using digital tools data science can strengthen disease management, as the country’s Covid-19 case study (FIND Digital Health Report, April 2021) shows.
This included integrating real-time surveillance and case management, aiming at more agile and efficient responses to future outbreaks.
Data in detail
Nigeria registered its first Covid-19caseon February 27, 2020.
Working closely with state health teams and partners, the Nigeria Centre for Disease Control (NCDC) led the response.
By March 29, 2021, more than 160 000 cases had been diagnosed from over 1.7-million tests.
Structure and data flow: SORMAS
The outbreak of Ebola resulted in the NCDC and partners developing Nigeria’s Surveillance, Outbreak Response Management and Analysis System (SORMAS).
This system expanded to support managing other priority diseases, including Covid-19, in January 2020, and was rapidly scaled up across Nigeria over the pandemic.
SORMAS is an end-to-end digital solution that captures geocoded data on all steps of the Test-Trace-Isolate cascade of Covid-19.
Using this tool,Nigeria has been able to capture data at multiple levelsto guide policy and programme interventions.
By 2021 Nigeria had several additional patient-facing tools, including:
The NCDC ChatBot accessed via the NCDC’s website
The self-assessment web application developed by Wellvis with NCDC
The Interactive Voice Response solution available as a call-back service
The USSD self-assessment solution
The Disease Control Hotlines established in many states.
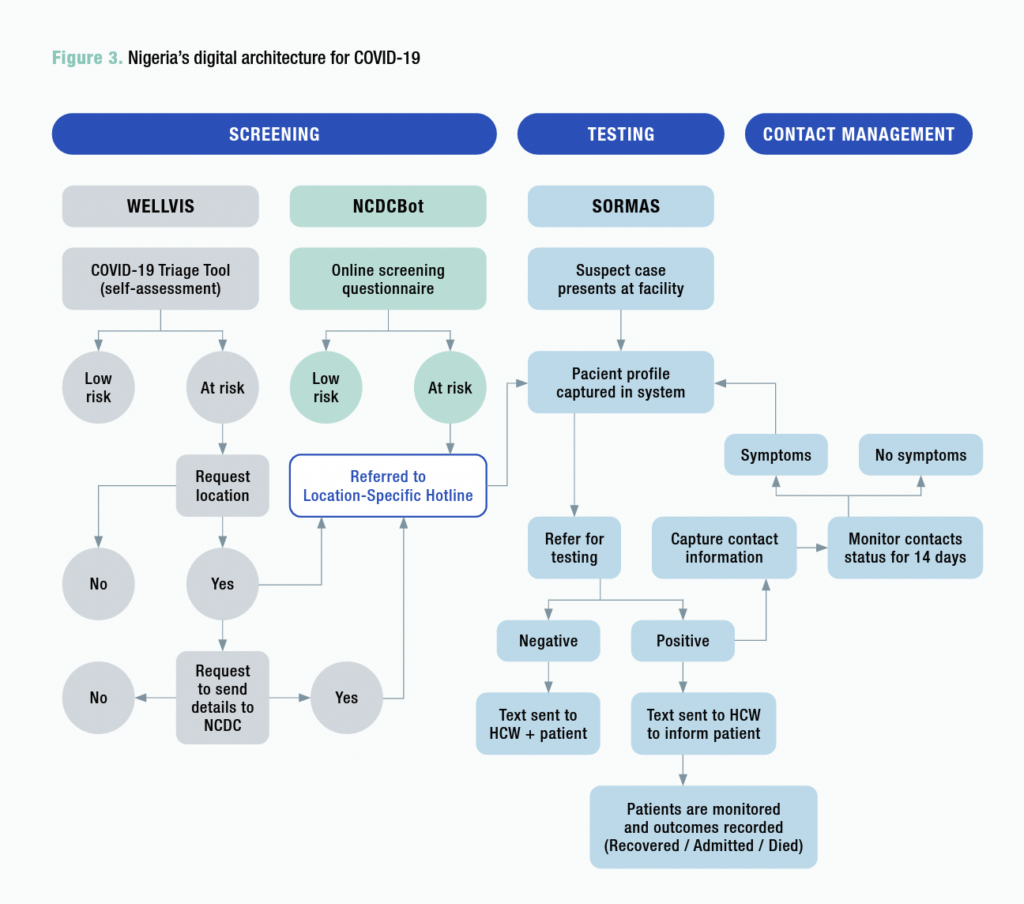
Covid-19 screening, testing and management
The graphic below shows how the NCDC ChatBot and Wellvis channels feed data to the dashboard, and to SORMAS, in the areas of screening, testing and management.
Why it works
Different dashboards are tailored to users at various levels of the health system
Data is transmitted to the NCDC website to provide to the public
Built-in algorithms generate early warnings for outbreaks, and SORMAS also generates data for surveillance and epidemiological analysis.
BENEFITS: Nigeria’s digital tools
Improvement in data quality
Better decision-making: SORMAS ensures all key demographic, epidemiological and clinical variables are recorded
Trigger warnings: users are notified of missing or incorrect key variables, preventing the next step until these are resolved
Central platform: routine recording of all metrics (test-trace-isolate phases) helps avoid additional data collection
Complete visibility: real-time supervision for health workers, motivating improved performance and guideline compliance.
Practical steps to develop scale
SORMAS was developed through a multi-institutional collaborationled by NCDC, the HZI, the African Field Epidemiology Network and German IT institutions. It transitioned from proprietary to open-source software in 2016 and its source code is accessible to software developers through the GitHub website.
In rolling out SORMAS, a training-of-trainers approach was used and, as new disease modules are added, this same approach is used.
Key success factors in Nigeria
Strong national ownership of SORMAS from the start.
As the NCDC actively promotes it as the preferred digital solution for Covid-19 management, there is less risk of multiple overlapping digital tools.
Integration into the broader health system, as it pre-dates the pandemic and was already in use.
“Design thinking” approach. SORMAS was responsive to the context in which the app was deployed, building on practical insights from the Ebola response.
Can be used offline. Data stored on the platform is automatically uploaded with connectivity.
Flexibility. A module-based approach means new ones can be rapidly added.
Operational challenges
One challenge is that mobile devices with old operating systems are unable to optimally support the SORMAS software.
Too few staff at implementation level can lead to delays in data being entered into SORMAS, negating the benefit of a real-time data capture system. However, the public should be able to input more data in the future, reducing the time taken by health care workers.
Key takeaways for other countries
SORMAS has led to improved data management and containment of the epidemic in Nigeria.
Ensuring automated data transmission between digital tools, and consolidating this using unique patient IDs, helps with comprehensive management of the pandemic.
Agility in digital tool development is vital, with continual changes to SORMAS to improve it.
Nigeria’s experience shows that integrating data into one platform enables better analysis of the cascade of care.
It also facilitates communication and referral between multiple players at different levels of the health system.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok